
Measuring the effectiveness of IQoro® treatment
Researching saliva control dysfunction in children and young people with Cerebral Palsy using practice-based evidence outcome measures
Research by Natalie Morris
Difficulty controlling saliva is a common problem for people with cerebral palsy (CP ). It is estimated that 500-2000 ml of saliva is produced each day and the average human being swallows 600 times a day.
Drooling is not normally a result of overproduction, but inefficient control of salivary secretions due to:
Inadequate lip closure / habitual open mouth posture
Reduced or impaired sensory feedback
Atypical muscle tone
Underlying swallowing difficulties
Dental problems
Side effects from other medications
My own clinical observations and experiences of working with children and young people with CP is that difficulty with saliva control is a persistent problem with no real effective treatment. The Cochrane review of interventions for drooling in children with cerebral palsy (Walshe M, Smith M, Pennington L 2012) concludes “There is no clear consensus on which interventions are safe and effective in managing drooling in children with CP. There is insufficient evidence to inform clinical practice on interventions for drooling in children with CP.”
NICE guidance on the assessment and management of CP in under 25s recommends clinicians assess factors that may affect drooling in children and young people with cerebral palsy, these include:
Compensatory strategies and management of contributory factors such as positioning – MDT working with OT and Physio to promote head control.
Increasing awareness of saliva – behavioural approaches to prompt children to swallow more often and wipe their faces. However, many people with CP have reduced sensory feedback and are often unaware that their chin is wet. Furthermore, the physical action of wiping their own chin can be difficult.
Oral-motor therapy – this aims to target musculature that can be voluntarily trained to improve muscle strength, tonicity and co-ordination. However, from a neurological point of view, it is important to consider that although some of our swallows are initiated during the conscious process of eating, drinking and specific exercises, the majority are reflexive: swallowing away our saliva without conscious involvement. The autonomic nervous system is responsible for the overall control of salivation. These nerves are not under conscious control.
Improving oral health - reducing reflux and maintaining good oral hygiene will reduce the bacterial load of saliva and reduce the risk of infection.
Eliminating mouthing behaviours - some tools that are provided to improve oral skills eg chewy tubes for jaw stability, can precipitate difficulties with saliva control, if used incorrectly and not as part of a structured program.

Most children and young people with CP are given some form of medication to help with saliva control. NICE produced guidelines in 2017 on the treatment of Hypersalivation in children with CP. The most common medications prescribed are:
Oral Glycopyrronium Bromide
NICE concludes there is moderate evidence for the effectiveness of this treatment, and no evidence for the long-term safety. Side effects include dry mouth, vomiting, constipation and thickening of secretions, which may increase the risk of respiratory infection and pneumonia. Many children are kept on this medication for years, at great cost to the NHS (NICE gives an average of £320 per bottle, around £430 for 28 days treatment, approx. £5160 per year).Hyocine patches + Trihexyphenidyl Hydrochloride
Although commonly prescribed, at the time of publication (January 2017), neither medication had a UK marketing authorisation for use in children and young people under 18 for treatment of hypersalivation.
Finally, if other treatment methods have been investigated, Botulinum Toxin injections into the salivary glands, or surgery to remove the glands may be considered. Although these would obviously be highly aversive experiences and considered only as a last resort.
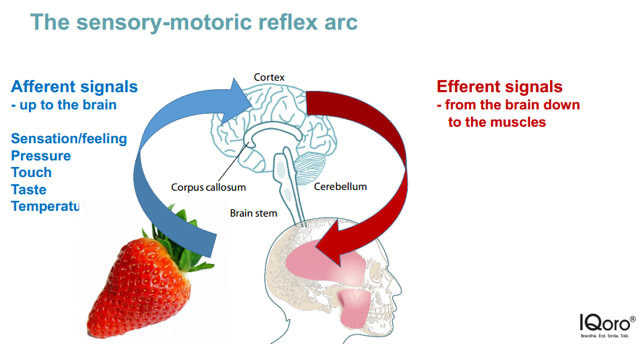
In 2018, I attended the ASLTIP conference and came across the IQoro®. The IQoro is a neuro-muscular training device that exercises and strengthens the muscles needed for feeding/swallowing and activates the nerve system to and from the brain. IQoro suggest that while traditional oral-motor therapy can target the musculature that can be voluntarily trained to improve muscle strength, tonicity and co-ordination, it does not target the two-thirds of the swallowing process that is controlled by the autonomic nerve system. IQoro claims to trigger the sensory-motoric reflex arc which enables messages to be sent to musculature beyond the reach of voluntary control. The sensory-motoric reflex arc effectively has a ’leveraging’ effect on direct muscular training and can improve the entire swallowing process.
Iqoro had a large amount of research that has been conducted on adults with aquired swallowining difficulties, but no evidence to support its use with children. The question that interested me was ”does the IQoro improve saliva control in children and young people with CP?” Over a 20 week period, I conducted a piece of practiced-based evidence to answer this question.
Method and design:
I used a case series design: 10 participants all had a primary diagnosis of CP, aged between 6-22 years old. A single case study design was applied to each individual and in addition to individual outcomes inferences were drawn from the collective data.
Several measures were taken to establish baselines, and these were compared to the measurements taken after the experimental phase.
I used a mixed method strategy, producing quantitative data regarding oral motor and swallowing ability + collecting qualitative data about how the patients / carers / MDT members perceived the value of the tool.
Data collection & Intervention:
Baseline assessments were taken of swallowing ability, oral motor function and speech. Rating scales were used that allowed for skill breakdown and functional description of each area.
The baseline assessment scores were used to set GAS Goals (Goal Attainment Scaling in Rehabilitation) for intervention.
An individual program for using the IQoro was designed for each patient and then carried out 3 x per day (by parents/carers) for 20 weeks.
Results
The composite GAS is transformed into a standardised measure with a mean of 50 - If goals are set in an unbiased fashion, one would expect a normal distribution of scores and the GAS thus performs at interval level. If goals have been fully achieved, we would expect to see a score of 50.
Figure 1: Results showing GAS scores pre and post treatment

Figure 2: Graphical representation of results

Discussion & Qualitative Analysis
In this study, it has been possible to demonstrate an improvement with saliva control resulting from treatment using IQoro. On average, ratings reduced from 4 (unable to control, saliva loss 75-100% of time) to 2 (moderate difficulty, saliva loss 25-50% of the time). However, at least half of the participants improved to a score of 1 (mild difficulty, saliva loss 10-25% of time).
Qualitative data reported (but not measured) saw improvements with: Teeth brushing; nasal breathing; breath control for speech; reduction in chest infections; sensory feedback (perception of saliva on chin) and tongue retraction. Positive feedback has been received from schools (less damage from saliva to IT equipment and worksheets) and Physio colleagues (able to work in supine for longer periods due to increase in swallowing of secretions).
Future plans include creating an assessment protocol and running a training program. Further research is indicated to see if this would be a cost-effective treatment that could be made available on the NHS.
Author
Natalie Morris // CEO & Founder // Speech & Language Therapist

References
Severe sialorrhoea (drooling) in children and young people with chronic neurological disorders: oral glycopyrronium bromide Evidence summary Published: 14 February 2017 nice.org.uk/guidance/es5
Interventions for drooling in children with cerebral palsy. Cochrane Database of Systematic reviews 2012, Issue 11 Walshe M, Smith M, Pennington L
Saliva Control in Children: An information guide for families and clinicians. Neurodevelopment and Disability The Royal Children’s Melbourne Hospital.
Goal Attainment Scaling (GAS) in Rehabilitation. A practical guide: Prof Lynne Turner Stokes, Regional Rehabilitation Unit, Northwick Park Hospital.